
New England Medicine in the Early 19th Century

Digging into Dr. Charles Knowlton’s background led me to several questions about the medical profession in the first half of the 19th century. During his life, Knowlton had trouble with the clergy, he spoke out against quackery, and he had several disagreements with neighboring (or competing) physicians. Some of his difficulties can be attributed to personality (he apparently wasn’t that easy to get along with) and beliefs (he was a fairly militant atheist). But I was left wondering about the profession. To what degree was medicine even a profession during Knowlton’s time? How did physicians view themselves? How did others view them? How effective were their methods, relative to available alternatives? If the results of doctors were no better than those of “quacks,” how did medicine manage to become a professional practice during this period?
One of the observations made by modern physicians about the medicine of the late eighteenth and early nineteenth centuries, is that it was dominated by a “preoccupation with system” (Lester S. King, M.D., Transformations in American Medicine From Benjamin Rush to William Osler, Baltimore: John Hopkins, 1991, 19). Drawing on the philosophical systematization of the universe by Descartes, Leibniz, Spinoza and Newton celebrated in the Scottish Enlightenment, medical doctors looked for all-inclusive conceptual systems that would explain all disease. Lacking knowledge of bacteria, viruses, and other causes of disease, doctors frequently treated the observable symptoms as disease itself. But I suspect their lack of data was exacerbated by a preference for comprehensive systems rather than limited, specific theories.
The goal of these systems was to make broad, universal generalizations out of observed facts. But the doctors’ preferences seem pretty clearly to have leaned toward the system rather than the supporting data. Benjamin Rush, for example, declared that facts, piled together, “would soon tumble to pieces, unless they were cemented by principles.” King compared this to Thomas Kuhn’s idea of paradigm creation in The Structure of Scientific Revolutions. The key difference, I think, was early doctors’ willingness to jump from limited data to universal explanations. “Their alleged facts,” King observed, “were in large part not facts at all, their reasoning not cautious but wildly speculative. But at the time this was not apparent” (King, 24). It’s ironic that one of the most successful and logically consistent “systems” of the nineteenth century was the completely erroneous technique of homeopathy (King, 22).
“The scientifically valid aspects of medical science” in this period, according to another medical textbook, “comprised gross anatomy, physiology, pathology, and the materia medica,” (William G. Rothstein, American Medical Schools and the Practice of Medicine, A History, New York: Oxford, 1987, 15). But there was a wide range of valid and invalid information contained in these broad categories. For example, although Rothstein said New England physicians around the turn of the nineteenth century used about 225 different drugs, he noted that “the range of action of these drugs was very limited” and that “the evacuants and opium were the most effective” (Rothstein, 16).
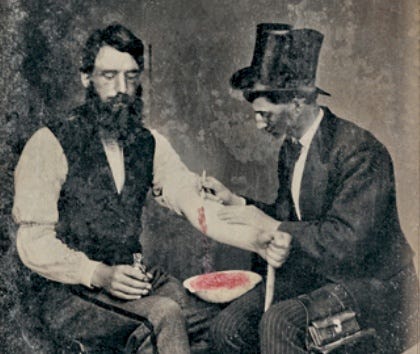
The often erroneous beliefs of New England doctors in the efficacy of their treatments were an important issue in their struggle to establish themselves as professionals. In retrospect, “the only drug of value in a wide range of illnesses was opium” (18), but opium was hardly the only drug New England doctors regularly prescribed. If many of their treatments were ineffective or even poisonous, as their critics claimed, then their success has to be attributable to something else. Skin irritation, for example, was a large part of many doctors’ prescriptive arsenal, on the belief that blistering would remove poisons from the body. A wide range of cantharides were used, all of which are now known to have been “of no medical benefit” (Rothstein, 17). The emerging profession’s stubborn insistence that their drugs were working and that their opponents’ treatments were not, was a major feature in their campaign for the public’s respect. The fact that the public was rightly skeptical of their claims probably impaired their message and delayed public acceptance of doctors’ unqualified authority on these issues.
Physicians’ very limited ability to observe only the surface symptoms of their (living) patients and to infer from impaired function, led them to classify most diseases as varieties of fever. A clearly-observable related symptom was inflammation, understood as a “local accumulation of blood” (King, 38). Phlebotomy (bleeding) was a logical treatment and was observed to reduce inflammation and fever at least temporarily. Drawing on this limited information, Benjamin Rush made an inductive leap and developed a unified theory of disease. All fever, Rush declared, was a “morbid excitement” of the blood vessels. Thus the doctor’s response to all disease should be the same. Rush’s heroic bleeding techniques called for the removal of enough blood to render the patient unconscious. In some cases, this meant regular bleedings of 16 to 24 ounces, until the patient recovered or died. Heroic bleeding wasn’t accepted by the public without some skepticism, even at the time. In 1800, William Cobbett remarked that Rush’s technique was “one of the great discoveries…which have contributed to the depopulation of the earth” (Alex Berman, “The Heroic Approach in 19th-Century Therapeutics,” Sickness & Health in America, Judith Walzer Leavitt & Ronald L. Numbers, eds., 77). Between 1797 and 1799, Rush successfully sued Cobbett for libel and was awarded the largest judgement of the time. Rather than paying, Cobbett returned to England.
In contrast to the grand theorizing of the “highly trained physicians of Edinburgh” like Rush, King observed that “poorly trained rural practitioners of New England” often attained a higher degree of “insight, discrimination, and critical judgment” (King, 79). He mentioned Dr. Nathan Smith, whose article on “Typhous Fever” he cited as an example of the new, more empirical medicine of nineteenth-century New England. Smith analyzed his data more critically and arrived at limited conclusions that “remained close to the observations” (86). But Nathan Smith, although he had begun his career as a Vermont village school-teacher, had also trained in London and Edinburgh. He founded the medical lectures at Dartmouth College that Charles Knowlton later attended. Rather than education, the key difference between doctors like Smith and their predecessors seems to be a scientific orientation that replaced an earlier, scholastic world-view. It’s interesting that physicians like Smith who embraced the specificity of science were precisely the men most opposed by conservative religious leaders like Timothy Dwight at Yale. Of course, most of them were also freethinkers.
The first New England medical schools were established in the 1760s in New York City and Philadelphia. Harvard’s first medical classes were offered in 1783 and in 1797 Nathan Smith began Dartmouth’s medical school as a one-man operation. Smith left Dartmouth in 1812 to help establish Yale’s program (over the objections of Dwight), and went on to participate in the founding of several other New England schools (for some reason, Rothstein de-emphasized Nathan Smith’s involvement, not even mentioning his name in connection with Dartmouth, where he was the “one-man” school Rothstein dismissively described. 29). But these medical schools were not “true academic departments” in the colleges they shared their names with. They were private businesses owned by their faculties, who received no support from the colleges and financed their operations on student tuitions. Nor were medical students usually drawn from the undergraduates of these colleges. At the beginning of the nineteenth century, a third of Yale or Dartmouth graduates became ministers. Another quarter became attorneys (Rothstein, 29). The ten percent of overall graduates who became doctors generally never associated with the other students at the colleges. They took none of the undergraduate classes and they had their own fourteen to sixteen week schedule of lectures, after which most returned to their preceptors, usually the doctor in their home-town, with whom the students were required to complete a three-year apprenticeship in order to earn their degrees.
King argued that the medical “elitism” that motivated the founding of the American Medical Association (AMA) in 1847 was partly ideological and partly economic (King, 210). The 1846 convention that resulted in the AMA’s formation addressed the competition of homeopaths and other “sectarians” in great detail. Complaining that “the community did not hold physicians in proper esteem,” the delegates discussed ways of establishing their profession on an equal footing with the other professionals they ran into in nearly every city and town, lawyers and clergymen. It's worth noting that these two professions were based on mastery of canonical texts (the Bible or legal tomes like Blackstone). How much did their desire to be favorably compared to these other men of the book, attorneys and ministers, influence physicians' reverence of an authoritative written tradition? Doctors distrusted "empirics", both within and outside their professional ranks. The Committee on Ethics called on AMA members to preserve their ideological purity by strictly refusing to give the “slightest countenance” to the “empirical imposture” of “presumptuous pretenders” (King, 211).
Sideways question... so often a good reveal of time and place.
Excellent piece... and not even finish it yet.